
From the 1Rehabilitation Medicine Center, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, and 2Children Rehabilitation Medicine Center, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan Province, China
Objective: To evaluate the prevalence of, and risk factors for, cerebral palsy in Henan province, China.
Methods: The prevalence of cerebral palsy in children aged 0–6 years between September 2011 and September 2012 was investigated using a stratified-clustered-random sampling method. An age-, sex- , and residence-matched control group of typically developing children was recruited. Univariate analysis and multinomial logistic regression analysis were used to identify risk factors associated with cerebral palsy.
Results: The prevalence of cerebral palsy in Henan province was 2.37 per 1,000 live births. Risk factors included: moving into a newly painted room; complicating maternal diseases (infection, heart disease, hypertension, anaemia, diabetes, kidney disease) during pregnancy; high gravidity (> 3); foetal asphyxia; low birth-weight (< 2,500 g); and hypoxic–ischaemic encephalopathy.
Conclusion: The prevalence of cerebral palsy in Henan province was 2.37 per 1,000 live births. Parents and clinicians should be aware of the risk factors for cerebral palsy.
Key words: prevalence; high-risk factors; rehabilitation status; cerebral palsy.
Accepted Aug 2, 2018; Epub ahead of print Oct 9, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Jianan Li, Rehabilitation Medicine Center, The First Affiliated Hospital of Nanjing Medical University, Nanjing 210029, Jiangsu Province, China. E-mail: lijianan@carm.org.cn
In this study, we investigated the prevalence of cerebral palsy in children aged 0–6 years old in Henan Province, Central China. Meanwhile, An age-, sex-, and residence-matched control group of typically developing children were recruited to identify risk factors associated with cerebral palsy. According to the epidemiological results,the prevalence of cerebral palsy was 2.37 per 1,000 live births, risk factors included moving into a newly painted room, complicating diseases (infection, heart disease, hypertension, anemia, diabetes, kidney disease) during pregnancy, high gravidity (> 3), foetal asphyxia, low birth weight (< 2,500 g), and hypoxic–ischemic encephalopathy.
C
erebral palsy (CP) describes a group of non-progressive neurological conditions that affect the foetal and infant brain (1–4). In developed countries, the prevalence of CP is approximately 1.4–2.9 per 1000 live births (2, 5–8). Liu et al. (9) reported a prevalence of 1.6 per 1000 live births based on a survey of 7 cities in China. Recently, with technological developments in healthcare, there has been a marked improvement in the diagnosis and treatment of CP in China.
In previous studies, researchers have proposed that high-risk factors for CP include asphyxia at birth, low birth-weight, and maternal infection (10, 11). It remains unclear whether factors such as age at pregnancy, socioeconomic status, and mode of delivery are associated with the prevalence of CP.
CP rehabilitation varies from country to country. Children with CP may go to special schools or ordinary schools and, in some developed countries, receive rehabilitation training in school (12).
A national registry of individuals with CP in China has not been established, and no large-scale epidemiological investigation of paediatric CP in the Chinese population has been conducted. Moreover current investigations of risk factors associated with CP in China are usually limited to a single-centre experience; large-scale analyses are sparse (13). Finally, rehabilitation status and educational opportunities are seldom reported in China. This study aimed to investigate the prevalence of, and risk factors for, CP in Henan province, central China.
The study was approved by the Institutional Review Board and ethics committee of the Third Affiliated Hospital of Zhengzhou University (2017AFZZ05). All caregivers (parents/guardians) provided written informed consent to participate with their children.
In order to investigate the prevalence of CP in Henan province, approximately 50,000 children aged 0 to 6 years 11 months were investigated. In this province, there are 18 cities, comprising 464 communities, and 108 counties, consisting of 1,892 townships. Eight cities and 1 community within each city were selected randomly. Twenty-six counties and 1 town within each county were also selected randomly. Each community was considered as an urban area sample, and each township as a rural area sample. All children who lived in these areas for more than 3 months, who were born between 1 January 2005 and 31 December 2010, were recruited. If more than one child resided in a given household, all the children in that household were recruited.
All children under 7 years of age in the selected areas were asked to undergo screening at a local hospital with paediatric physicians or neurologists who had received specialized training. The screening was in 2 phases: enquiry about medical history and motor development history to gather information about motor development delay; and physical examination to determine whether there were abnormal movement, posture, reflex, muscle tension and muscle strength and whether motor development was normal. In order to be cautious and comprehensive, if either motor development delay or physical examination was positive, the screen was regarded as positive. Children who screened positive were asked to undergo diagnosis 10 days later with another senior paediatric physician or neurologist. They were examined and referred for further examination, such as magnetic resonance imaging (MRI) of the head, electromyography, etc., as appropriate. Potential cases of CP, or subjects who could not be diagnosed or excluded, were referred to senior paediatric neurologists or rehabilitation specialists in the local hospitals.
CP diagnostic criteria: (i) persistent central movement disorder; (ii) abnormal movement, posture and reflex; (iii) abnormal muscle tension and muscle strength; (iv) the symptom was caused by non-progressive brain damage sustained as a foetus or infant.
CP exclusion criteria: (i) transient development delay; (ii) hereditary metabolic disease with motor dysfunction, such as metachromatic leukodystrophy, dopa-responsive dystonia, Duchenne muscular dystrophy, or myotonic muscle dystrophy; (iii) presumed insult to the brain, specific and occurring after birth (e.g. an intracranial haemorrhage caused by late-onset vitamin K or craniocerebral trauma).
Matched control group: All children in the control group were recruited from the same areas during the same screening period (from September 2011 to September 2012). Each child with CP was matched with 4 typically developing controls, according to location (community or town), age (± 3 months), and sex.
Data collection was undertaken between September 2011 and September 2012. Caregivers and paediatric rehabilitation practitioners were requested to jointly complete the risk factor questionnaire. Items in the questionnaire pertaining to potential risk were devised by a Delphi procedure. Firstly, 20 renowned paediatric rehabilitation experts were asked to list the risk factors for CP and to classify the risk factors according to their clinical experience via e-mail. Based on the results, a preliminary questionnaire was constructed, which was then returned to the 20 experts for further advice. Analysis, statistical treatment, and modification of the questionnaire were carried out, and minor events were elaborated further. The questionnaires included 3 concepts: (i) maternal, prenatal and gestational risk factors; (ii) perinatal risk factors; and (iii) postnatal risk factors/neonatal diseases. Questions included parental age at conception, educational level of parents, mean household income, location of residence, contact history of parents with physical and chemical agents, moving into a freshly painted room for 6 months or more during pregnancy, family history of genetic diseases, maternal concomitant diseases during pregnancy, maternal medication history, the nutritionl status of the mother, frequency of ultrasound scanning during pregnancy, whether an X-ray examination or computed tomography (CT) scan was performed, maternal alcohol consumption during pregnancy, maternal active or passive smoking during pregnancy, preconception irregularity of menstrual cycle, gravidity and parity, abortion times, foetal times, history of abnormal pregnancy, and vaginal bleeding during pregnancy; (ii) perinatal risk factors, including completed weeks of gestation, mode of delivery, dystocia, abnormalities in progression of labour, birth asphyxia (based on medical record at birth),and birthweight; and (iii) postnatal risk factors/neonatal diseases, including neonatal hypoxic–ischaemic encephalopathy (HIE), neonatal seizures, infection, and jaundice.
Birth-weight was classified into 3 groups: <2,500, 2,500–4,000 and > 4,000 g. Gestational age was classified into 3 groups: < 37, 37~42 and ≥ 42 weeks. Pregnancies were classified as singleton or multiple. Parental age was classified into 3 groups: ≤ 25, 25–30 and ≥ 30 years. Educational level of parents was classified into 5 groups: illiteracy or elementary school, junior middle-school, senior middle-school, university, and post-graduation or higher education. Residence type was classified as urban or rural. Gravidity was classifed into 3 groups: First gravidity for the current birth, the second
time, and multigravidity (≥ 3 times); parity was classifed into 3 groups: primiparity for the current birth, the second time, and multiparity (≥ 3 times).The latter result was consistent with the grouping. Household income per capita was classified as <10,000 and ≥ 10,000 Chinese yuan. History of contact with physical and chemical agents was defined as > 6 months contact history with pesticides such as propoxur (aryl carbamate), dimethoate (dithiophosphoric acid, o-dimethyl-s ester), decorative materials such as emulsion paint (e.g.polyvinyl acetate latex paint) and glue (e.g. plywood), benzene (C6H6), mercury, arsenic and chemical solvents (e.g.methanol ), all these explore time was more than 4 days per week, and 7 hours per day). History of contact with X-rays was defined as ≥ 3 times or more. Active or passive maternal smoking status was classified into 3 groups: 0, 1–2 and ≥ 3 cigarettes per day. Mode of delivery was dividing into vaginal delivery or caesarean section. Abortion data were classified into 3 groups: 0, 1 and ≥ 2 abortions. Data were independently entered into Epidata Entry version 3.2 (EpiData Association, Odense, Denmark) by 2 separate investigators. Medical records were consulted when necessary, if available.
Statistical analyses were conducted using Stata (version 12.0; STATA Corp., College Station, TX, USA). Conditional logistic univariate and multivariate regression analyses were performed to detect potential risk factors. For the univariate logistic regression analyses, alpha was set at p < 0.10. Significant risk factors were submitted to multivariate regression analysis. Bivariate odds ratios and 95% confidence intervals (95% CIs) were calculated. Alpha was set at 0.05.
A total of 50,596 children (age range 9–81 months), from a population of 51,266 eligible children, were included in the analysis. The other children were not screened (1.31%). Of the included children, none of the parents or guardians refused permission for their children to enter the study. There were 23,040 females and 27,556 males (female:male 1:1.196). Of these, 822 children screened CP-positive. Further examination resulted in 235 being diagnosed as normal, 436 were diagnosed with transient developmental delay, 26 with intellectual disability, 5 with muscular torticollis, and 120 with CP. Thus, the true positive rate of the screening was 14.60%.
Regarding CP, the prevalence was 2.37% (95% CI) 1.95–2.79). There were 76 boys and 44 girls with CP. The prevalence in male children was 2.76% (95% CI 2.14–3.37%) and in female children 1.91% (95% CI 1.34–2.47%), respectively. The χ2 test showed no significant difference in prevalence between sexes (p > 0.05).
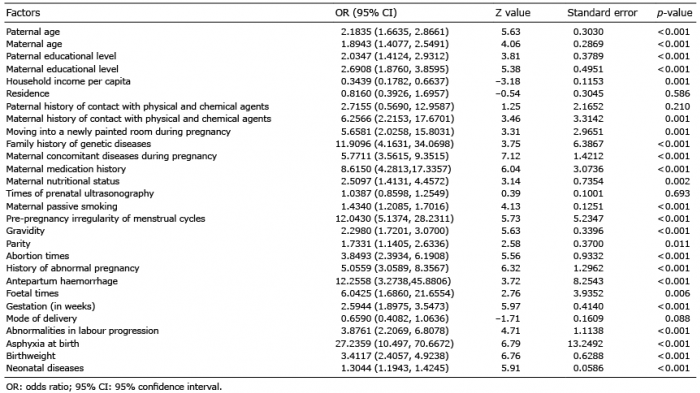
The following factors were excluded from the analysis as they were reported less than 1% of the time: maternal alcohol intake during pregnancy, X-ray examination or computed tomography scanning during pregnancy, maternal active smoking, and dystocia. The statistical results of the univariate logistic regression analyses are summarized in Table I.
Table I. Statistical results of univariate logistic regression analyses
The variables showing a significant correlation with the occurrence of CP in univariate logistic regression analyses (p < 0.10) were included in the multivariate logistic regression analysis. For ordinal data, scatterplots were created with the independent variable on the x-axis and probability of having CP on the y-axis. Scatterplots of parental educational levels and maternal education levels did not reveal a rectilinear trend. Therefore, educational level was transformed into a categorical variable and included in the multivariate logistic regression analysis. However, scatterplots of maternal passive smoking, abortion times, and the nutritionl status of the mother, showed significant rectilinear trends, and these factors were analysed directly in the multivariate logistic regression analysis. The scatterplots are presented in Fig. 1.
Fig. 1. Relationship between risk factors and probability of having cerebral palsy (CP) for ordinal data.
Statistical results from the multivariate logistic regression analysis are summarized in Table II. The results reveal that the following are high-risk factors for CP:moving into a newly painted room, complications with concomitant diseases(including diabetes, hypertension, anemia, heart disease, kidney disease) during pregnancy, high gravidity (≥ 3), asphyxia (severe respiratory depression at birth, the effective spontaneous breathing didn’t creat afer 1 minute from birth and Apgar score is less than 7; umbilical artery blood gases analysis: Ph<7.15), low birth weight (< 2,500 g), and HIE.
This cross-sectional study was a census of children under 7 years old recruited from 24 districts and towns in 24 cities in China. The prevalence of CP was 2.37 per 1,000 live births (95% CI 1.95–2.79%). This is the frst large-scale study to estimate the prevalence of CP in China, since a study
published in 1997 of the prevalence of CP in Jiangsu province (13). In the 1997 study, the epidemiology results revealed that the prevalence of CP in childhood (age < 7 years) was 1.6 per 1,000 live births, which was significantly lower than in the present study. The higher prevalence found in our study can be attributed to advances in obstetric and neonatal rescue techniques, since many infants with very low birth-weight and gestational age less than 28 weeks now survive. This interpretation is consistent with Liu et al.’s finding that the prevalence of CP documented in their 1997 study increased continually over the study period (9). In 2013, Oskoui et al. (7, 8) conducted a meta-analysis comprehensively analysing data on the prevalence of CP collected since 1985. The overall prevalence was estimated to be 2.11%, which is similar to our findings.
In the current study, the true positive rate (TPR) of screening was 14.60%, the main reason for the low TPR was the wide standard for positive screening. The diagnostic results proved this: 235 were regarded as normal, and 436 were diagnosed with transient transient developmental delay, out of 822 children who were regarded as positive in the screening.
CP prevalence in male and female children was 2.76% and 1.91%, respectively, according to our study. A χ2 test indicated that this difference in prevalence between sexes was not significant. The relationship between sex and prevalence of CP remains controversial. Some researchs, the present study included, have found no statistically significance between male and female (14–16). However, some other studies have found a higher prevalence of CP in male than female children (14, 17, 18). The exact relationship between sex and prevalence may vary considerably in different districts. Further research, including much larger sample sizes, will be needed to elucidate the relationship between sex and CP prevalence.
The present study implicated neonatal asphyxia, moving into a newly painted room, complication with maternal concomitant diseases during pregnancy, high gravidity (≥ 3), low birth-weight (< 2,500 g), and HIE to be risk factors for CP.
Studies have found that CP-related risk factors include low socioeconomic status (6), gestational diabetes, maternal infection (19), low gestational age, multiple births, family history of genetic diseases, breech presentation, antepartum bleeding, multiple miscarriages, smoking, illicit drug use (18), etc. (9, 20, 21). In a previous study, Garfinkle et al. analysed outcomes for neonates with suspected asphyxia using the Canadian Cerebral Palsy Registry. They noted that neonatal asphyxia was significantly correlated with CP (22). Sukhov et al. (20) conducted a retrospective population-based cohort study of children registered in California over a 10-year span. They found that premature birth was a major risk factor for CP, and that neonatal asphyxia and adverse intrapartum events contributed significantly to the development of CP (20). Low birth-weight was also considered a risk factor for CP (1, 23). In the current study, low birth-weight (< 2,500 g) was identified as a statistically significant risk factor in both univariate and multivariate analysis. However, premature birth (≤ 37 weeks) did not reach statistical significance. Beaino et al. reported similar findings (24). The definitive effects of intrauterine growth retardation on cerebral development are undetermined at present.
In the current study, high gravidity (≥ 3) was identified as a high-risk factor, whereas parity was not significant. Similarly, in a previous systematic review by McIntyre et al., there was no significant association between parity and CP (25). A possible explanation for this could be that gravidity was confounded with the number of abortions and maternal gestational age; mothers with high gravidity (≥ 3) were relatively older and usually had experienced multiple miscarriages.
Pollutants, such as formaldehyde and benzene, in decorative materials may impair neonatal cerebral development. Recently, other studies have found that moving into a newly decorated room during pregnancy is associated with congenital disease, such as congenital cardiovascular disease, Formaldehyde may cause the permanent damage to the brain and kidneys of the pregnant mother and benzene may cause the feotus malformation, especially in the first trimester-the the critical stage of fetal organ formation, although further research is needed (26). Some authors have proposed that plurality may be a risk factor for CP (18, 27). However, in the current study, no statistically significant evidence was detected.
In order to reduce the risk of CP, measures should be taken to maintain a healthy lifestyle, mothers should not move into a newly painted room, and healthcare personnel should be aware of neonatal asphyxia, low birth-weight, and HIE in children. If neonatal asphyxia or HIE is found, early intervention is recommended.
In conclusion, this is the first large prevalence study of CP since 1997 in China, and the first of risk factors for CP in a geographically defined area of China. The study further elucidates CP in China and provides some suggestions for preventing CP.
The current study has some limitations, however. The number of children investigated was limited and some high-risk factors did not have abundant sample sizes. As a cross-sectional epidemiological investigation, Gross Motor Function Classification System level 1 (GMFCS-1) CP might be omitted because of atypical clinical manifestation when the children were young, especially spastic hemiplegia, which means that the prevalence of CP may be under-represented.
This work was supported by grants from the Health Industry Special Scientific Research Project (grant number 201002006) and the Henan provincial science and technology research project (grant number 201203053).
We thank the paediatricians, rehabilitation physicians, and staffs in Zhengzhou, Xinxiang, Zhumadian, Kaifeng, Sanmenxia, Shangqiu, Luohe, Puyang, Luoyang cities who helped in the epidemiological investigation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize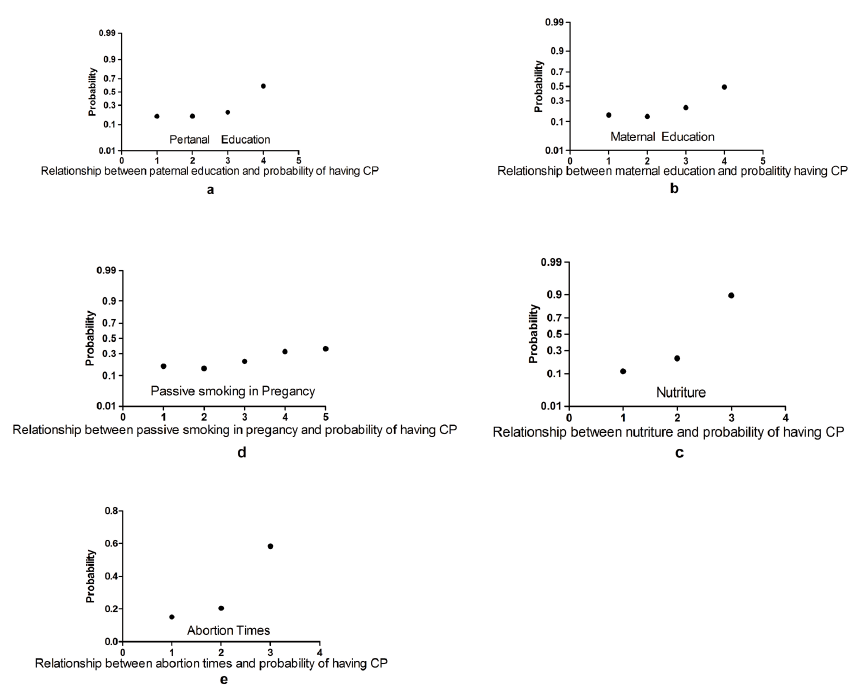 Click to show fullsize
Click to show fullsize